This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those clinical problems with collective current best evidence based inputs.
A 57 yr old male patient resident of gopalayapalli came to opd with chief complaints of generalised edema and decreased urine output since one month, chest pain since 4 days.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic one month back later he developed swelling of face followed by abdomen and limbs which is pitting type since one month.
He had decreased urine output since one month.Intially there was dribbling of urine later there was complete stoppage of urine.
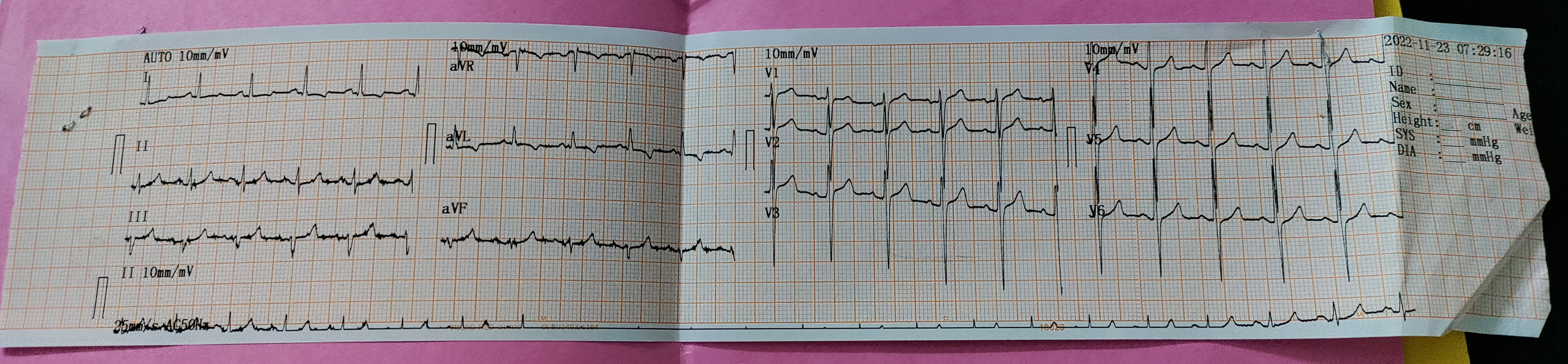
He had chest pain since 4 days which was sudden in onset, dragging type,radiating towards back,and aggravated at night.
H/o fever associated with chills,on and off type since one month.
H/o shortness of breath (grade 3)
H/O cough associated with sputum since one month and not relieved on medication.
It is not associated with chest pain and no diurnal variation.
Sputum is blood tinged.
He had 9 sessions of dialysis (on alternate days) from one month recent one was yesterday.(23/11/22)
PAST HISTORY:
He is diabetic since 15 yrs.He is using gluconorm and since one month he is on insulin.(because of his flucutating blood glucose levels)
He had Hypertension since 5 yrs and he is under medication.
No H/o epilepsy,CAD,Asthma.
No H/o surgeries in past.
No allergic history.
FAMILY HISTORY:
His mother and father are hypertensive.
PERSONAL HISTORY:
Diet:Mixed
Appetite:Normal
Sleep: Adequate
Bowel and bladder movements: Decreased urine output and had constipation.
Addictions: Alcoholic since 15 yrs stopped one month back
Smoker since 30 yrs and stopped 20 yrs back.
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative.
Moderately built and nourished.
No signs of icterus,cyanosis, clubbing, lymphadenopathy.
He had generalised edema( pitting type),pallor.

Vitals:
SYSTEMIC EXAMINATION:
Respiratory system:
Bilateral air entry-present ,
Normal vesicular breath sounds-heard.
Cardiovascular system:
S1 and S2 heard no murmurs heard
Central nervous system:
No focal neurological deficit.
Patient is concious coherent.
Higher mental status-
Cranial nerves- intact
Motor system:
Tone- normal
Power- normal
Cerebellar functions-normal
Abdominal examination:
soft and non tender,
No Hepatomegaly, spleen is not palpable.
INVESTIGATION:









Comments
Post a Comment